Giving Youth a Voice in Therapy

Giving youth a voice in therapy is given a lot of lip service. But just like privileging clients, when the doors are closed or the teletherapy begins, whose voice is really heard? This is especially true with children and adolescents, since they are most likely to be “volunteered” for therapeutic services by someone else. And it is especially true about the young person’s perspective of the benefit and experience of therapy.
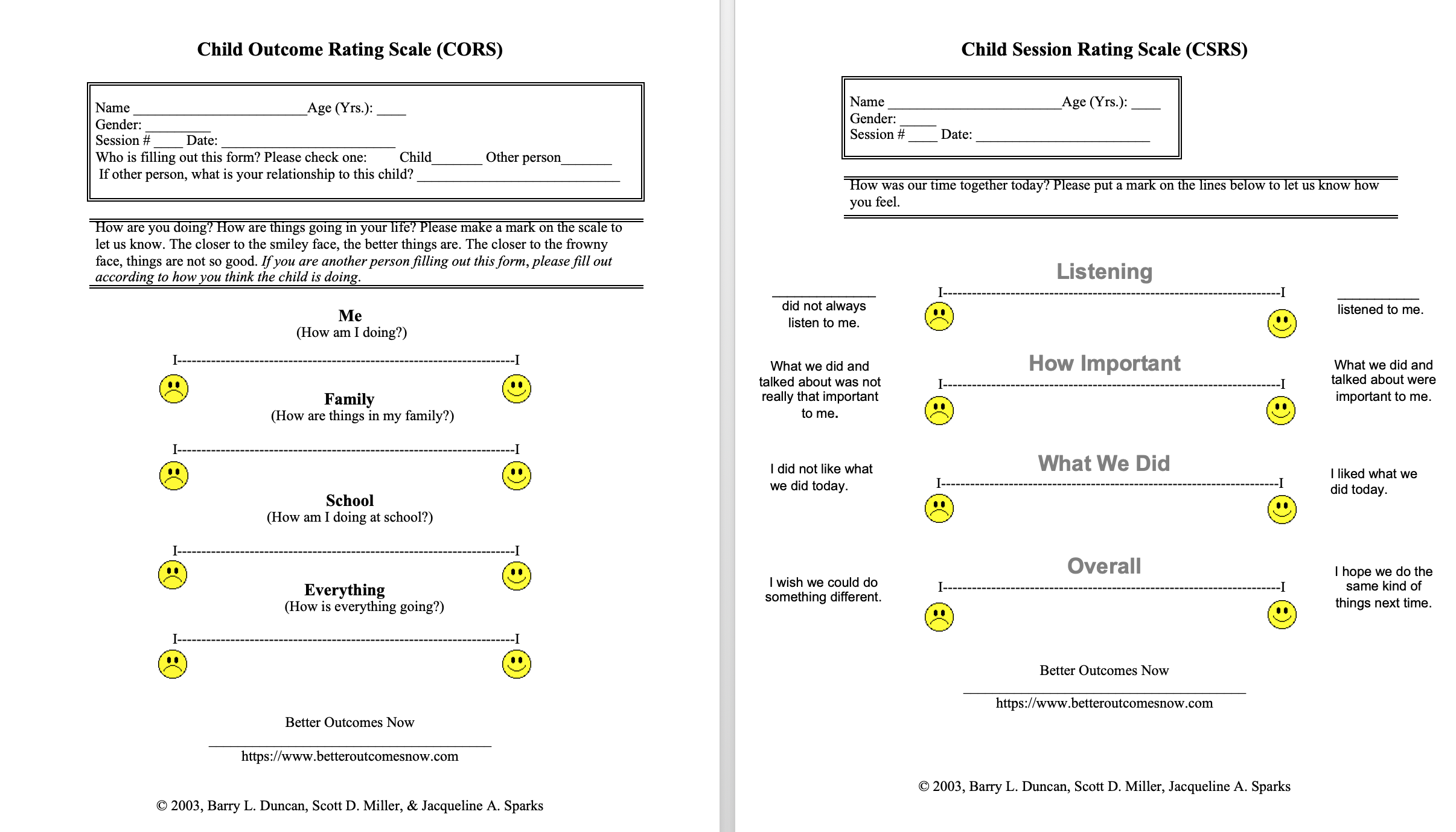
Ensuring that young people have a voice in therapeutic services is why the Child Outcome Rating Scale and Child Session Rating Scale were developed. They are the first self-rated mental health outcome measures and therapeutic alliance measures for children 12 and under. Apparently, before then, the field didn’t care so much about what the youth thought of the therapy they received.
Child Outcome Rating Scale & Child Session Rating Scale: A Little History
After the Outcome Rating Scale and the Session Rating Scale were co-authored and I developed the clinical process of the Partners for Change Outcome Management System (PCOMS), first delineated in the original PCOMS manual, Heroic Clients, Heroic Agencies: Partners for Change (Duncan & Sparks, 2002), my friend and colleague Dr. Jacqueline Sparks and I sought to expand the benefits of client privilege to youth and their families — and the Child Outcome Rating Scale and Child Session Rating Scale were developed.
The clinical process with youth and their families was first described in the second edition of Heroic Clients, Heroic Agencies (Duncan & Sparks, 2007) as well as in Brief Intervention in the Schools, a book with my longtime friend, Dr. John Murphy (Murphy & Duncan, 2007).
Giving Youth a Voice in Therapy: The Research
Thanks to two ground-breaking clinical sites (the Center for Family Services of Palm Beach County, Inc. in West Palm Beach, Florida and Southwest Behavioral & Health Services in Phoenix, Arizona) and two PCOMS visionaries and longtime friends (Dave Claud and Dr. Bob Bohankse), the Child Outcome Rating Scale and the Outcome Rating Scale were psychometrically validated for use for children and adolescents. Next came demonstrating that PCOMS made a difference in youth outcomes.
Dr. Sparks, with colleagues in the UK, published a cohort study that reported significantly better results for children, parents, and teachers. This was followed by a benchmarking study (again thanks to the great Bob Bohanske) that found similar outcomes to randomized clinical trials with youth who had PCOMS included in their services.
Finally, a pilot randomized clinical trial conducted in the UK as a prelude to a much larger study (under way) with children 7-11 found significantly better outcomes. You can read more here about these studies conducted by the Better Outcomes Now team or download the .PDFs from the Science of PCOMS resource center.
The Clinical Process: Everyone Has a Voice
PCOMS represents a departure from expert-driven formulations that attempt to classify client distress and problems of living from a theoretical or symptom vantage point. Instead, clients are empowered to highlight their views of distress/well-being, refocusing therapy toward individualized problem construction and solution building and away from options based on diagnosis, symptomology, or normative functioning. In work with youth and families, PCOMS includes a desire to learn each person’s perspective about the presenting concerns, the benefits of service, and the therapeutic alliance.
The logistics of PCOMS administration with youth and families should feel familiar to therapists accustomed to the complexity of family work (read 5 Tips for Using Outcome Measures with Families). A major value of PCOMS in systemic work is its capacity to initiate conversations about discrepant views in objective, non-blaming ways. The therapist’s inquiry about the differences in Child Outcome Rating Scale (CORS) or Outcome Rating Scale (ORS) scores sets the stage for developing mutual goals and a means to measure success. Effective navigation by the therapist of these differences should be reflected in Child Session Rating Scale (CSRS) or Session Rating Scale (SRS) ratings, allowing the therapist a chance to recalibrate ongoing work accordingly.
The transparency of the PCOMS process establishes a space where all views are respected and meanings are co-explored; continuous responsiveness to clients’ unique views, grounded in valid, objective data, fosters dialogue, the emergence of mutual solutions, and a built-in safety net for avoiding treatment failure.
Read more about implementing PCOMS with young people and families in the new PCOMS manual.